A lumbar synovial cyst is a small fluid-filled sac that appears next to a facet joint of the spine. Often it causes no symptoms, but if it compresses a nerve root it can cause leg pain, tingling, cramps or difficulty walking. The important thing is not to be alarmed by the word “cyst”: in most cases it is not a tumor nor does it imply cancer, but it can act as a mechanical cause of sciatica or lumbar stenosis.
- A lumbar synovial cyst is often related to wear of the posterior joints of the spine.
- It can be an incidental finding on an MRI or cause symptoms if it narrows the canal or compresses a nerve.
- Symptoms can closely resemble those of a herniated disc or lumbar stenosis.
- Treatment depends on symptoms, nerve compression, instability and response to conservative management.
- Surgery is reserved for selected cases, especially if there is disabling pain, neurological deficit or failure of non-surgical treatment.
What is a lumbar synovial cyst
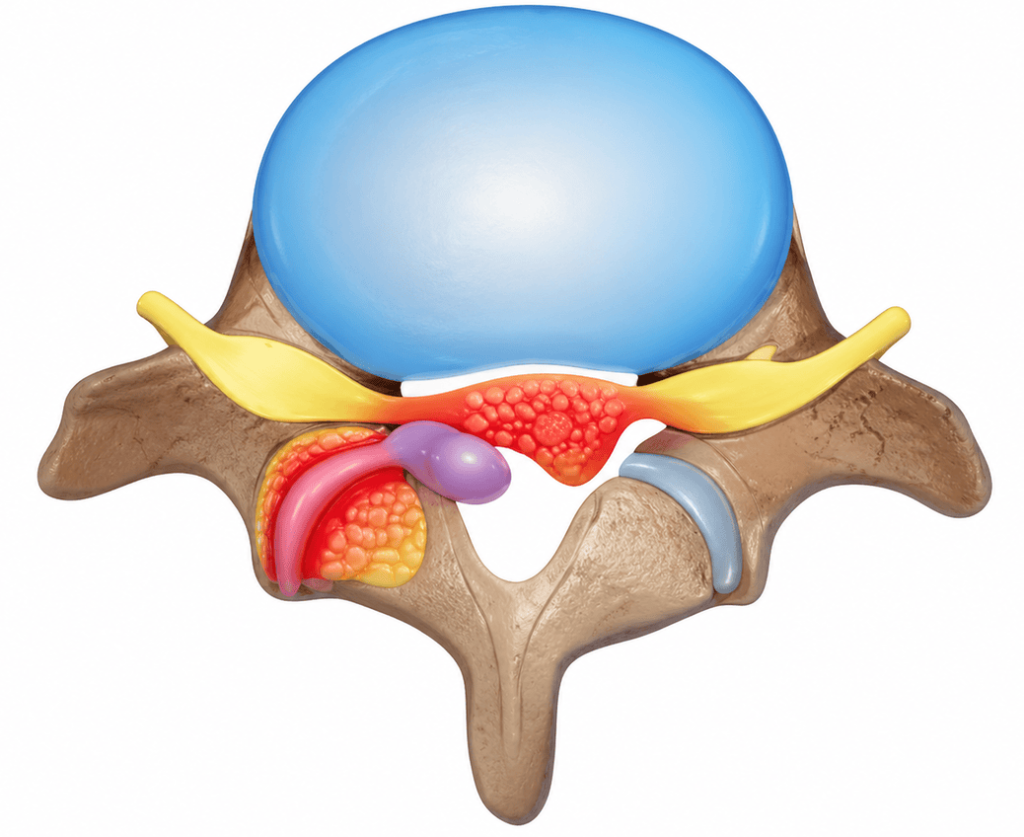
The lumbar spine has small joints at the back called facet joints. They help guide movement and provide stability. Over the years these joints can degenerate, become inflamed or produce more synovial fluid than usual. That fluid can accumulate and form a sac: the synovial cyst.
The term can be frightening, but it is worth clarifying from the start: a lumbar synovial cyst is usually a benign lesion. The problem is not that it is “malignant”, but the space it occupies. If the cyst grows toward the lumbar canal or toward the foramen where the nerve exits, it can compress nervous structures.
That is why some people have a synovial cyst and notice nothing, while others develop low back pain, sciatica, numbness or weakness. The difference lies in size, location, associated inflammation and whether there is stenosis, facet arthropathy or spondylolisthesis, which is the slipping of one vertebra over another.
8 signs your sciatica may not come from a herniated disc
1. Leg pain that worsens when standing
A common clue is pain that appears or increases when standing or walking, and improves when sitting or bending forward. This is similar to lumbar stenosis because, by changing posture, the available space for the nerves also changes.
2. Tingling or numbness in one leg
If the cyst compresses a nerve root, tingling, numbness or an electric sensation can appear in the buttock, thigh, leg or foot. The specific area depends on the nerve involved.
3. Pain that does not entirely match a typical herniated disc
A herniated disc is usually associated with a disk protruding and compressing the nerve. In a synovial cyst, compression comes from the posterior joint. The symptom can be similar, but the cause is not the same. That is why MRI is so important when the pain does not improve or neurological signs appear.
4. Low back pain with facet arthropathy
The cyst often appears in a context of facet joint wear. It may be accompanied by mechanical low back pain, stiffness, discomfort when extending the back or pain that changes with posture.
5. Cramping or heaviness when walking
Some patients describe their legs “getting heavy” when walking and needing to sit to recover. This can be confused with circulatory problems. The key is to assess whether it improves when flexing the spine, for example when leaning on a shopping trolley.
6. Symptoms in flares
The size and tension of the cyst can fluctuate. Some people have better and worse weeks. That does not mean the problem is imaginary, but that compression and inflammation can vary.
7. History of spondylolisthesis or instability
Synovial cysts are sometimes associated with microinstability of the lumbar segment. If one vertebra moves more than expected, the facet joint can become irritated and contribute to cyst formation.
8. Pain that returns after injections or medication
Anti-inflammatories, analgesics or injections can relieve symptoms for a time, but if the main cause is persistent compression, symptoms may recur. This does not automatically mean surgery is required, but it does require reviewing the diagnosis.
How it is diagnosed
Medical history and examination
Diagnosis begins by listening to the pain pattern: where it starts, where it radiates, which postures worsen it, how far the patient can walk and whether there is loss of strength or sensation. The examination checks reflexes, strength, sensation, gait and maneuvers that point toward a nerve root problem, hip, sacroiliac joint or facet pain.
Magnetic resonance imaging (MRI)
Lumbar MRI is the most useful test to see a synovial cyst, its relationship with the nerve roots and whether there is canal or lateral recess stenosis. It also allows checking for herniated disc, facet arthropathy, inflammation or degenerative changes at other levels.
Dynamic X-rays
In some cases flexion and extension X-rays are requested. They serve to assess whether instability exists. This information is important because it can change the strategy: it is not the same to remove an isolated cyst as to treat a segment that also moves abnormally.
CT scan or complementary studies
CT can provide bony detail, especially if there is marked arthropathy, calcification or for surgical planning. Neurophysiological studies can help if there is doubt between a lumbar radiculopathy and other peripheral neurological problems.
Treatment alternatives
Non-surgical options
If symptoms are mild, there is no loss of strength and quality of life is reasonably preserved, conservative treatment can be considered. This includes education, activity modification, active physiotherapy, lumbopelvic control exercises, cautious pain relief and follow-up.
Physiotherapy does not necessarily “dissolve” the cyst, but it can improve load tolerance, reduce mechanical irritation and help the person move with less fear. The goal is not absolute rest, but adapted activity.
Injections
Injections can be used to reduce inflammation or to confirm the source of pain. In some cases an attempt is made to aspirate or decompress the cyst using image-guided techniques, although results can vary. If the cyst is thick, septated or the compression is significant, the response may be limited.
Surgical decompression
When leg pain is disabling, there is clear compression on MRI or conservative treatment fails, surgical decompression may be considered. The goal is to remove the cyst and free the nerve root. In selected cases this can be done via less invasive approaches, depending on the anatomy, cyst size and the team’s experience.
Decompression with fusion
Not all cysts require fusion. Fusion is considered when there is instability, significant spondylolisthesis, deformity, important mechanical pain or the need to remove structures that could destabilize the segment. The decision must be individualized because adding fusion can reduce recurrence in some profiles, but it also increases the magnitude of the surgery.
Benefits, risks and adverse effects
Expected benefits
In a well-selected case, freeing the nerve can reduce radiating pain, improve walking ability and decrease tingling or cramps. When the main symptom is root compression, improvement in the leg is usually more predictable than improvement of mechanical low back pain.
Possible risks
Like any procedure, injections and surgery carry risks. These can include infection, bleeding, reaction to medication, transient worsening of pain, nerve injury, cerebrospinal fluid leak, cyst recurrence or the need for further surgery. In a fusion there are added risks related to implants, bone healing and adjacent levels.
Limitations
MRI can show several findings at once: herniation, arthropathy, stenosis, cyst and disc wear. The challenge is to identify which finding actually explains the symptoms. Operating on a finding that is not the main cause of pain can lead to poor results, even if the technique is well performed.
Criteria for referral or specialist assessment
It is advisable to consult a specialist if leg pain does not improve after several weeks of well-guided treatment, if it limits walking, if there is persistent tingling, if MRI shows nerve compression or if there is doubt between herniation, stenosis, hip, sacroiliac or vascular problem.
Assessment should be faster if there is new loss of strength, falls, progressive pain, bilateral symptoms or prior lumbar surgery. It also deserves careful review if the MRI report mentions a synovial cyst, severe stenosis or spondylolisthesis.
Realistic recovery times
With conservative treatment, recovery is measured in weeks or months. There can be progressive improvement if irritation decreases and there is no severe compression. In selected cases some cysts may stabilize or even reduce, although this should not be assumed as usual.
After an injection some people notice relief within days, while others barely improve. The effect can be temporary. If decompression surgery is performed, many people walk the same day or the next, but full recovery depends on the prior state of the nerve, age, musculature, other diseases and whether fusion was added.
As a rough guide, light activities can be resumed within weeks after a simple decompression, while a fusion requires longer timeframes, often several months to consolidate strength, mobility and confidence. Return to work depends heavily on whether the job is sedentary or physical.
When to go to emergency
Seek urgent care if there is sudden loss of strength in a leg, new difficulty walking, loss of bladder or bowel control, numbness in the genital or perineal area, unbearable pain with fever, or low back pain after major trauma. These symptoms are not typical of simple sciatica and require immediate evaluation.
Myths and realities
Myth: “If it says cyst, it’s cancer”
Reality: a lumbar synovial cyst is usually benign. The problem is mechanical, due to compression or inflammation, not oncological.
Myth: “Every cyst must be operated on”
Reality: if it does not cause symptoms or symptoms are mild, it can be observed or treated conservatively.
Myth: “If the leg hurts, it’s always a herniation”
Reality: sciatica can be due to herniation, stenosis, synovial cyst, foraminal narrowing or other causes.
Myth: “MRI decides on its own”
Reality: imaging must match the symptoms and examination. An MRI without context can lead to wrong conclusions.
Frequently asked questions
Is a lumbar synovial cyst dangerous?
In most cases it is not dangerous in terms of malignancy. It is usually benign. It can be relevant if it compresses nerves and causes pain, weakness or walking limitation.
Can it disappear on its own?
It can occur in selected cases, but it should not be assumed. The decision to observe or treat depends on symptoms, examination and the compression seen on MRI.
Can it be confused with a herniated disc?
Yes. Both can cause sciatica. The difference is the structure compressing the nerve. That is why MRI and clinical correlation are essential.
Can physiotherapy cure it?
Physiotherapy does not always eliminate the cyst, but it can improve pain, mobility, strength and tolerance to activity. It is reasonable for mild to moderate symptoms without progressive neurological deficit.
Can an injection prevent surgery?
Sometimes it can relieve enough to avoid or delay surgery. In other cases the effect is partial or temporary. It depends on the cyst’s size, content and location, as well as the nerve compression.
When is surgery needed?
Surgery is considered if there is disabling pain, neurological deficit, significant difficulty walking, clear compression or failure of conservative treatment. The decision must be individualized.
Is fusion always necessary?
No. Fusion is considered if there is instability, relevant spondylolisthesis, deformity or risk of destabilizing the segment during decompression.
Can it come back?
There is a possibility of recurrence, especially if facet degeneration or instability persists. That is why the full context of the lumbar segment is evaluated.
Glossary
- Synovial cyst: fluid-filled sac related to a synovial joint.
- Facet joint: posterior joint of the spine that guides part of vertebral movement.
- Sciatica: pain that runs down the leg due to irritation or compression of nerve roots.
- Lumbar stenosis: narrowing of the canal or the spaces through which the nerves pass.
- Radiculopathy: symptoms produced by involvement of a nerve root.
- Spondylolisthesis: slipping of one vertebra over another.
- Decompression: surgery intended to free compressed nerves.
- Fusion or arthrodesis: surgery that joins two or more vertebrae to stabilize a segment.
Medical references consulted
The following sources were used as documentary basis to prepare this educational content on lumbar synovial cyst, sciatica, lumbar stenosis, imaging diagnosis and treatment options.
- NICE. Low back pain and sciatica in over 16s: assessment and management. 2016, reviewed in 2020. https://www.nice.org.uk/guidance/ng59
- American Association of Neurological Surgeons. Lumbar Spinal Stenosis. https://www.aans.org/patients/conditions-treatments/lumbar-spinal-stenosis/
- NCBI Bookshelf. Lumbar Spinal Stenosis. StatPearls, updated 2024. https://www.ncbi.nlm.nih.gov/books/NBK531493/
- NCBI Bookshelf. Facet Joint Disease. StatPearls, updated 2025. https://www.ncbi.nlm.nih.gov/books/NBK541049/
- NCBI Bookshelf. Lumbosacral Facet Syndrome. StatPearls, updated 2025. https://www.ncbi.nlm.nih.gov/books/NBK441906/
- Benato A, et al. Decompression with or without Fusion for Lumbar Synovial Cysts: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 2023. https://pubmed.ncbi.nlm.nih.gov/37048747/
- Benato A, et al. Decompression with or without Fusion for Lumbar Synovial Cysts: full text in PMC, 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10095101/
- Ganga A, et al. Optimizing surgical management of facet cysts of the lumbar spine: systematic review, meta-analysis, and local case series. Journal of Neurosurgery: Spine, 2023. https://pubmed.ncbi.nlm.nih.gov/37728373/
- Hassan M, et al. Spontaneous resolution of synovial lumbar cyst presented with severe symptoms. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11403793/
- Matsoukas S, et al. Comparative evaluation of surgical techniques applied in the treatment of lumbar synovial cysts: systematic review and meta-analysis. 2025. https://pubmed.ncbi.nlm.nih.gov/40029066/
Health disclaimer: this content is educational and does not replace an individual medical assessment. If you experience progressive symptoms, loss of strength, changes in sphincter control, fever or unusually severe pain, seek medical attention.