Pseudarthrosis means a spinal fusion has not healed (fused) as expected. Sometimes it causes no symptoms, but when it does, it often shows up as “mechanical” pain (worse with load) or a feeling of instability. The good news is that, with an accurate diagnosis, there are options: from improving fusion healing and managing pain to considering revision surgery in selected cases.
- Pseudarthrosis is a failure of the bone to fuse after a fusion surgery.
- It doesn’t always hurt, but it can explain persistent pain or implant failure.
- Diagnosis is not based on a single test: the combination of symptoms, exam, and imaging matters.
- Smoking, older age, and multi-level fusions increase the risk.
- There are non-surgical treatments (bone health optimization, rehab, stimulators in specific cases) and surgical options (revision).
- If new weakness, high fever, or loss of bowel/bladder control appears, seek emergency care.
What pseudarthrosis is and why it happens
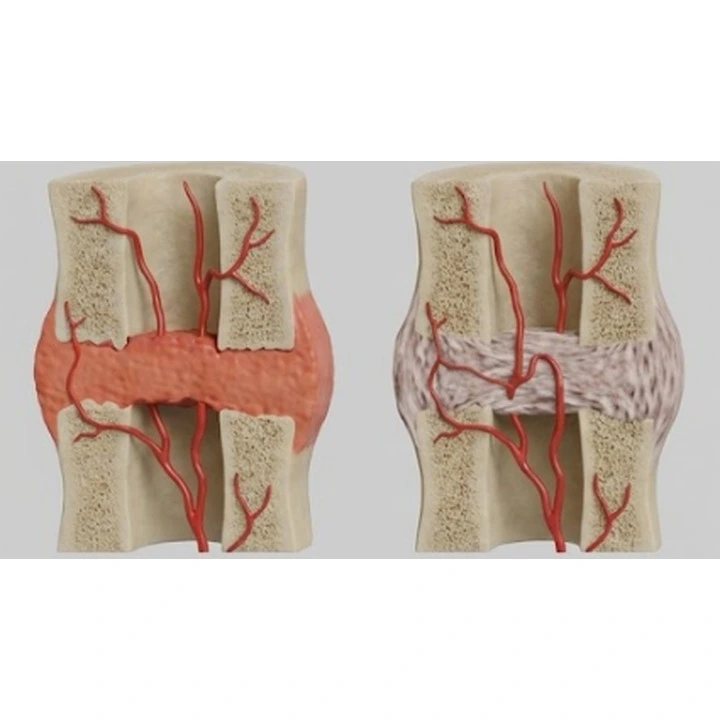
In a fusion (arthrodesis), the goal is for two or more vertebrae to heal together as one solid bone, eliminating painful motion at that segment. We call it pseudarthrosis when that bony bridge does not mature or fails to form completely. In simple terms: the body “doesn’t fully weld” the operated area.
Two key points to understand:
- Not all pseudarthrosis causes symptoms. It may appear on imaging while the person feels fine.
- Not all pain after fusion is pseudarthrosis. There are many other causes (irritated nerve, sacroiliac joint, facet joints, scar tissue, neuropathic pain, etc.).
9 signs that may suggest pseudarthrosis
These signs don’t confirm anything on their own, but they do justify a focused clinical and imaging review:
1) “Mechanical” pain that worsens with load
More pain when standing, walking, climbing stairs, carrying bags, or at the end of the day, with relative relief at rest.
2) Early improvement followed by worsening months later
Some people feel better in the first weeks, but between months 3 and 12 notice pain returning or plateauing.
3) A sense of instability or “not feeling solid”
Not everyone experiences this, but when it occurs it is often described as feeling unsafe when twisting, bending, or changing positions.
4) Pain localized to the operated segment
A more focal pain at the surgical level, different from nerve pain that travels down the leg or arm.
5) Clicking or discomfort with certain movements
It’s not always significant, but if it comes with progressively worsening pain, it should be assessed.
6) Pain that doesn’t follow the expected recovery pattern
After a fusion, some discomfort, stiffness, and fatigue are normal. The red flag is when pain doesn’t improve at all over time or clearly worsens despite reasonable rehab.
7) Worsening with coughing, sneezing, or straining
This can happen due to increased pressure and tension in the area. It’s not specific, but it adds information.
8) Indirect signs of hardware failure
In some cases, pseudarthrosis is associated with loosening or breakage of screws/rods. This doesn’t happen every time, but when it does, it often comes with progressive mechanical pain.
9) Persistent pain with real functional impact
When pain prevents basic activities (walking, sleeping, working) and there’s no other clear explanation, ruling out a nonunion is advisable.
How to diagnose it reliably
Diagnosing pseudarthrosis is a puzzle built from symptoms, physical exam, and imaging. The key is avoiding two extremes: “everything is pseudarthrosis” and “it can’t be that.”
Clinical evaluation
- Where the pain is and what triggers it.
- Whether pain is mainly mechanical, nerve-related, or both.
- Neurologic check: strength, sensation, reflexes, and gait.
Most commonly used imaging tests
- X-rays in different views to assess alignment and hardware.
- Dynamic X-rays (flexion-extension) to evaluate abnormal motion in some cases.
- CT scan to assess the bony bridge and fusion quality (often the most useful test when there is doubt).
- MRI if nerve compression, infection, or other associated issues are suspected.
One important detail: sometimes imaging looks “borderline,” but if the person feels well and functions normally, observation may be appropriate. And the opposite can happen too: a CT may show signs of nonunion while the main pain generator is something else (for example, the sacroiliac joint or neuropathic pain).
Risk factors: what you can change and what you can’t
Pseudarthrosis is multifactorial. These factors are frequently seen in studies and in clinical practice:
Factors you CAN’T change
- Age: risk increases over time.
- Number of fused levels: the more extensive the fusion, the more demanding the healing process.
- Underlying condition: deformities and complex surgeries tend to carry higher risk than a short, straightforward fusion.
Factors you CAN improve
- Tobacco or nicotine: smoking is linked to poorer fusion healing. Quitting before and after surgery improves outcomes.
- Bone health: osteoporosis or low bone density increases mechanical complications and makes fusion harder.
- Nutrition: low protein intake, vitamin D deficiency, or poor overall health can affect healing.
- Poorly controlled diabetes and other metabolic issues: they can interfere with recovery.
- Extreme inactivity: appropriately dosed movement and well-structured rehab usually help.
Non-surgical alternatives: what may help
Not every suspected case ends up in the operating room. It depends on symptoms, daily-life impact, stability, and progression.
1) Set expectations and monitor timelines
Bone healing is slow. In many fusions, the process can take months. In selected cases, follow-up with pain control and rehabilitation can be appropriate.
2) Active rehab and “smart loading”
The goal is neither “endless rest” nor “pushing through.” What often helps is:
- Progressive daily walking.
- Adapted strengthening of the trunk and hips.
- Learning to move with confidence, using good technique.
3) Optimize bone health
In people with low bone density, assessment and treatment to improve bone quality are commonly recommended before or after surgery, depending on the clinical context. This may reduce the risk of screw loosening and improve the fusion environment.
4) Multimodal pain management
The aim is to restore function without relying solely on medication. This can include non-opioid analgesics, treatment for neuropathic pain when appropriate, and sleep and activity strategies.
5) Bone growth stimulators (in selected cases)
Some stimulation devices may support fusion healing in people at high risk or with suspected nonunion. They’re not for everyone and are prescribed based on clinical and imaging criteria.
Surgical options: when revision is considered
Revision surgery may be considered when there is:
- Significant persistent pain with functional limitation that doesn’t improve with reasonable measures.
- Imaging confirmation of nonunion that matches the clinical picture.
- Hardware failure, progressive deformity, or instability.
- Associated nerve compression that explains symptoms.
What revision surgery aims to achieve
- Improve the biological environment for fusion (graft, bone preparation).
- Increase stability (revise or extend instrumentation if needed).
- Address contributing problems (residual stenosis, alignment, etc.).
A revision doesn’t always mean “massive surgery,” but it is usually more demanding than a first operation. That’s why a precise diagnosis matters so much.
Benefits vs risks and possible side effects
Potential benefits
- Less mechanical pain when nonunion is the main cause.
- Improved function (walking, standing, working) in well-selected cases.
- Greater stability and lower risk of ongoing hardware failure.
Possible risks and adverse effects
- Infection, bleeding, blood clots, wound-healing problems.
- Persistent pain (especially when multiple pain sources coexist).
- Nerve injury, cerebrospinal fluid leak, or need for further surgery.
- Slower recovery than after a primary procedure.
The decision should be based on an honest balance between what can likely improve and what cannot be promised.
When to seek referral and helpful second opinions
A specialist evaluation is advisable if:
- Mechanical pain is progressively worsening after 3-6 months with clear impact.
- Hardware failure or a worsening deformity is suspected.
- There is new radiating pain or a neurologic deficit.
- Tests don’t match the symptoms and you need a clear plan.
A good second opinion doesn’t repeat tests “by routine,” but focuses on answering: what hurts, why it hurts, and which option makes the most sense right now.
Realistic recovery timelines
Timelines depend on whether management is conservative or surgical, and on how many levels are involved. As a general guide:
- Conservative follow-up: functional improvements may appear within weeks, but bony healing (if progressing) is assessed over months.
- After fusion revision: the first month is often an adaptation phase with gradually increasing walks; between 6 and 12 weeks, independence improves; full recovery may take several months.
More than an exact date, what matters is a staged plan: pain under control, walking more, rebuilding strength, returning to work, and then resuming leisure and sport when it’s safe.
When to go to the emergency department
Seek urgent care if any of these symptoms appear:
- New or progressive weakness in a leg or arm.
- Loss of bladder or bowel control, or numbness in the genital/perineal area.
- High fever with chills and worsening pain, or a draining wound.
- Unbearable pain that doesn’t ease and comes with neurologic symptoms.
- Breathing difficulty or painful swelling of one leg.
Myths vs reality
- Myth: “If I have pseudarthrosis, I’ll definitely need another surgery.” Reality: not always. It depends on symptoms, stability, and progression.
- Myth: “If it hurts after a fusion, the surgery went wrong.” Reality: pain can have multiple causes, and many are treatable without more surgery.
- Myth: “One test confirms everything.” Reality: diagnosis is clinical and radiologic, not a single data point.
- Myth: “If I stop smoking one week before, that’s enough.” Reality: the longer you’re nicotine-free before and after, the better for fusion healing.
Frequently asked questions
Does pseudarthrosis always hurt?
No. It can exist without symptoms. When it does cause symptoms, it’s often mechanical pain or progressively reduced function.
What is the best test to confirm it?
In many cases, a CT scan is particularly useful for evaluating fusion, but it’s always interpreted alongside symptoms and other imaging.
When is a fusion considered “not healed”?
There isn’t one universal timeline. Often, progress is assessed between 6 and 12 months, depending on symptoms and follow-up findings.
Does quitting smoking really change anything?
Yes. Nicotine is associated with worse bone healing. Quitting beforehand and staying nicotine-free afterward improves prognosis.
Can it be fixed without surgery?
Sometimes, especially if symptoms are mild and the segment is stable. Optimizing bone health, rehab, and supportive measures may help in selected cases.
Does revision surgery guarantee the pain will go away?
No guarantee is possible. It can improve symptoms if pseudarthrosis is the main cause, but results may be partial if other pain sources coexist.
What’s the difference between nerve pain and mechanical pain?
Nerve pain often travels along the nerve path (down a leg or arm) with tingling or burning. Mechanical pain is usually more localized and worsens with load or movement.
What signs mean it’s an emergency?
New weakness, loss of bowel/bladder control, high fever with worsening pain, or numbness in the genital/perineal area.
Glossary
- Arthrodesis (fusion): surgery that joins vertebrae to stabilize them.
- Pseudarthrosis: failure of bone healing after an attempted fusion.
- Mechanical pain: pain that worsens with load and improves with rest.
- Radicular pain: pain that radiates along a nerve (e.g., into the leg).
- Dynamic X-rays: flexion-extension views used to assess motion.
- CT scan: computed tomography, useful to evaluate the bony bridge.
- Revision: surgery to correct a problem from a prior operation.
References
- Lumbar fusion pseudarthrosis risk factors: systematic review and meta-analysis (PMC) – 2024
- Effectiveness of electrical stimulation for spinal fusion (Scientific Reports) – 2020
- Radiographic assessment of successful lumbar spinal fusion (Scoping review, PMC) – 2025
- Pseudarthrosis and reoperation risk: a systematic review (PMC) – 2024
- Revision surgery outcomes for pseudarthrosis after lumbar fusion (Global Spine Journal) – 2020
Educational notice
This article is for informational purposes and does not replace individualized medical advice. If you have worrying symptoms or neurologic changes, contact a healthcare professional promptly or go to the emergency department.